
Tongue Reconstruction
- Home
- Tongue Reconstruction
About Tongue Reconstruction
Tongue reconstruction is a surgical procedure to rebuild the tongue after part (or all) of it is
removed — most often due to oral cancer.
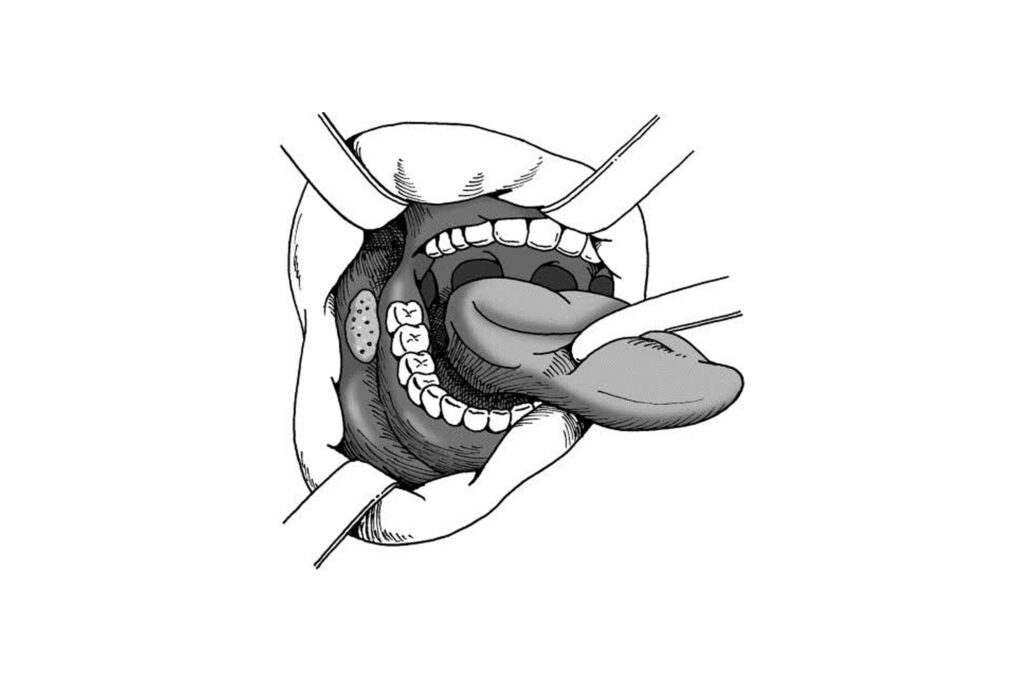
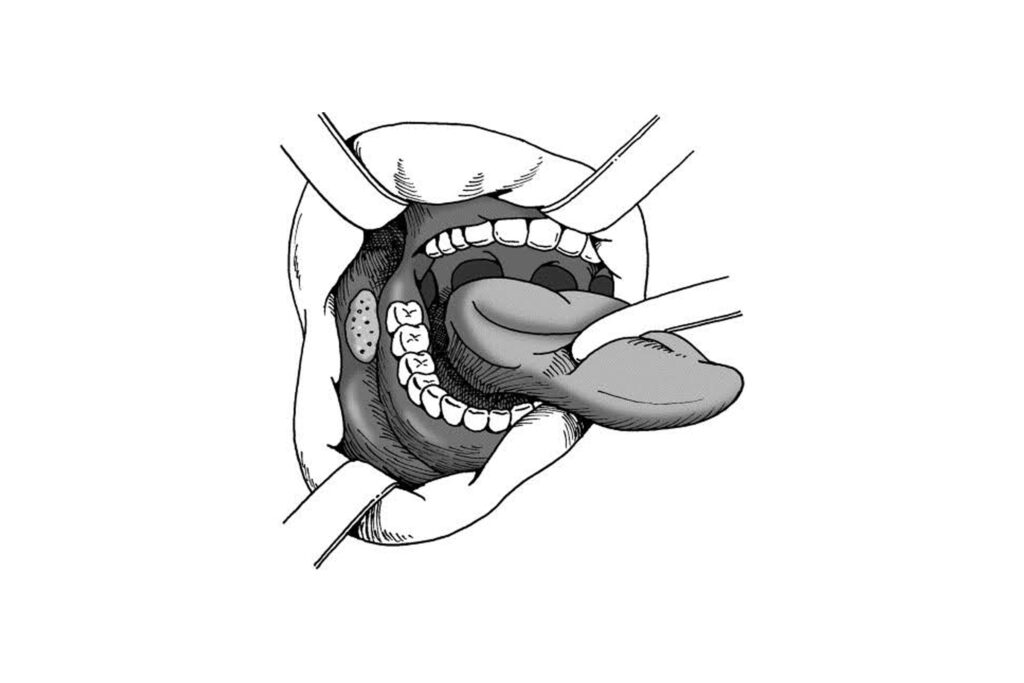
When cancer affects the tongue, surgeons may perform a partial or total glossectomy (removal of part/all of the tongue). This creates a defect that can affect:
To restore these vital functions, reconstructive surgery is performed using tissue from another
part of the body.
Goals of Tongue Reconstruction:
- Restore mobility of the tongue for speech clarity
- Enable safe swallowing and chewing
- Maintain or restore oral aesthetics
- Ensure airway protection and breathing
- Help patients return to a normal lifestyle
Tongue reconstruction can be done using the following flaps
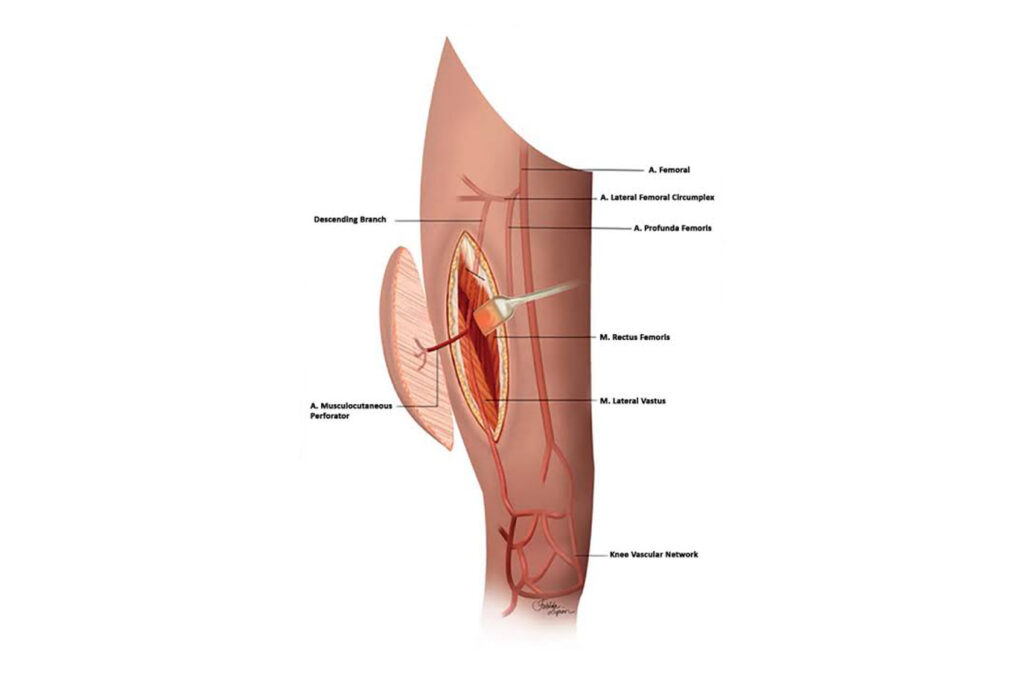
Tongue Reconstruction Using a Free Anterolateral Thigh (ALT) Flap
What is a Free Anterolateral Thigh (ALT) Flap?
- “Free flap” means tissue is taken from one part of the body and moved to another with its
blood supply reconnected using microsurgery. - The ALT flap is taken from the outer thigh. It includes skin, fat, and sometimes muscle,
ideal for rebuilding soft tissues like the tongue.
Why is the ALT flap used for tongue reconstruction?
- Large Size: Provides a broad skin area to match tongue defects.
- Low Donor Site Problems: The thigh heals well with minimal visible scarring.
- Customizable Thickness: Can be made thin or thick based on patient needs.
- Reliable Blood Supply: Helps the flap survive and heal well.
Step-by-Step Process :
1. Tumor Removal:
Surgeon removes the tongue cancer (partial/hemiglossectomy or total).
2. Flap Harvesting:
Tissue is taken from the outer thigh along with its artery and vein.
3. Microsurgery:
Flap’s blood vessels are connected to neck vessels under a microscope.
4. Shaping the Tongue:
The flap is trimmed and shaped to resemble the tongue’s contour.
5. Donor Site Closure:
Thigh wound is either closed directly or with a skin graft.
What will the patient experience?
- Hospital stay: Usually 4–6 days
- A feeding tube (Ryle’s tube) inserted via the nose may be used at first to maintain nutrition.
- Speech and Swallowing therapy: Begins early to help adapt to the new tongue.
- Scarring: Minimal on the thigh flap inside the mouth blends over time.
- Function: Good results in restoring speech, swallowing, and tongue movement.
Summary:
*The Anterolateral Thigh (ALT) flap is a reliable, versatile option for tongue reconstruction after cancer surgery. The flap is customizable in thickness, has a good blood supply, and leaves minimal visible scarring at the donor site. Ideal for medium to large defects, it offers excellent functional outcomes with rehabilitation.
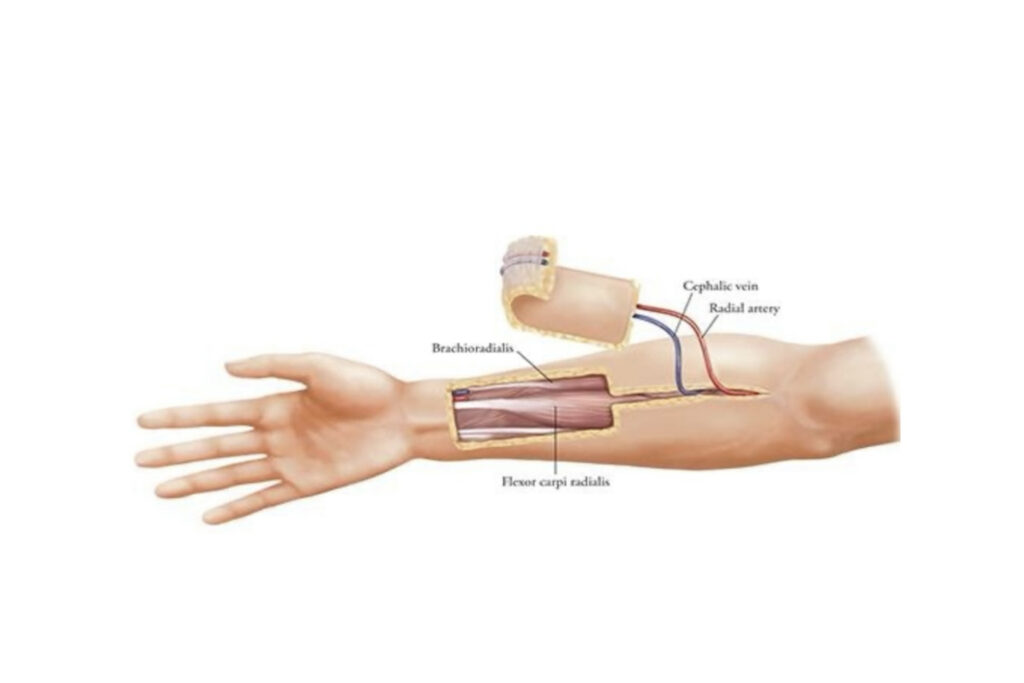
Tongue Reconstruction Using a Free Radial Artery Forearm Flap (FRAFF)
What is a Free Radial Artery Forearm Flap?
- It is thin, flexible tissue taken from the inner forearm.
- Includes skin, fat, and the radial artery for blood supply.
- Transferred to the tongue area, where the artery and vein are reconnected to neck vessels using microsurgery.
Surgical Steps (Simplified):
1. Tumor removal
(glossectomy or hemiglossectomy)
2. Harvesting
forearm tissue with artery & vein
3. Microsurgical transfer
to the mouth and reconnecting vessels
4. Shaping
the flap to resemble tongue structure
5. Donor site closure
(usually with a skin graft from thigh)
Patient Recovery & Expectations:
- Hospital Stay: 4-5 days
- A feeding tube (Ryle’s tube) inserted via the nose may be used at first to maintain nutrition.
- Donor Site: A scar on the forearm (covered with graft)
- Therapy: Speech and swallowing rehab begin early
- Functionality: Good speech and swallowing in most cases
Summary:
*The Free Radial Artery Forearm Flap is ideal for medium-sized tongue defects where mobility and flexibility are essential. It is one of the most time-tested and successful techniques in tongue reconstruction.
Tongue Reconstruction using Medial Sural Artery Perforator (MSAP) Flap
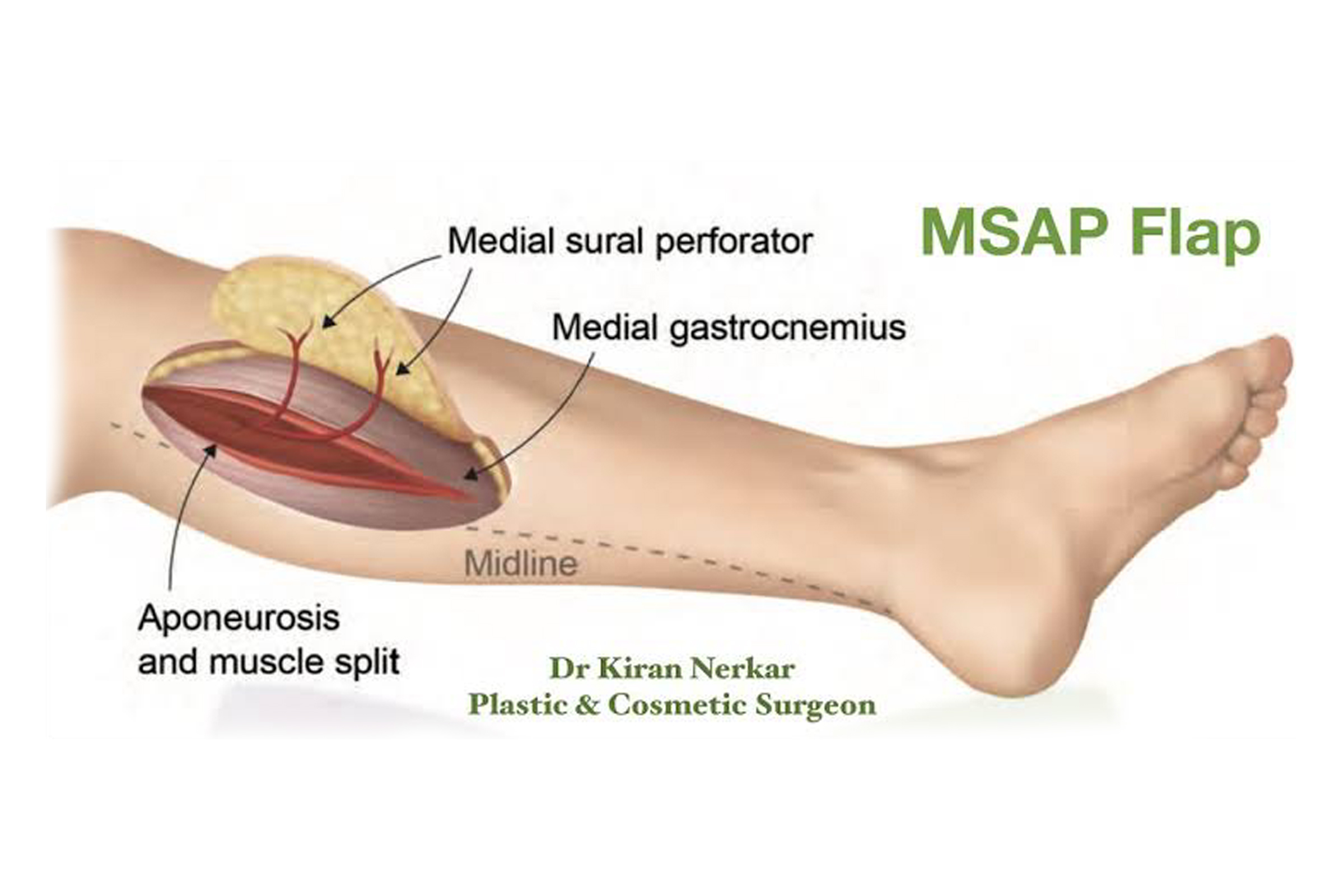
What is the MSAP Flap?
The Medial Sural Artery Perforator (MSAP) flap is a thin, pliable tissue flap taken from the
back of the lower leg (calf area). It includes skin and fat, nourished by small perforator branches
of the medial sural artery
Why Use It for Tongue Reconstruction?
- Thin & flexible – closely mimics tongue texture
- Ideal for small to moderate defects.
- Hidden donor site – scar is on the back of the leg.
- Better cosmetic result than forearm flap
- Reliable blood supply via microsurgical technique
How It Works :
1. Tumor is removed from the tongue
2. MSAP flap is harvested from calf
3. Vessels are connected to neck vessels under microscope
4. Flap is shaped to reconstruct part of the tongue
5. Donor site is closed primarily or with skin graft
Patient Benefits:
- Maintains speech and swallowing function
- Less visible scarring compared to forearm donor site
- Good esthetic and functional outcome in experienced hands.
Best For:
- Small to medium-sized tongue defects
- Patients wanting better cosmesis than forearm flap
Tongue Reconstruction Using a Nasolabial Flap
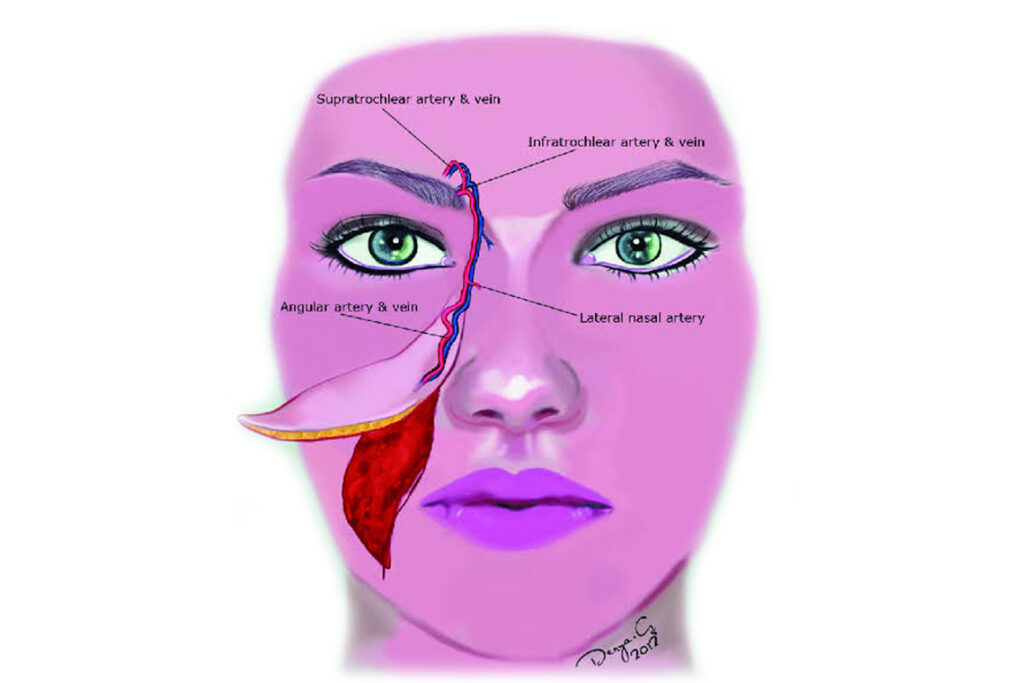
What is a Nasolabial Flap?
A nasolabial flap is a local flap taken from the cheek area, near the fold between the nose and
the corner of the mouth (the nasolabial fold). It is a pedicled flap, meaning it stays attached to
its original blood supply during transfer.
Why is it used for tongue reconstruction?
- Simple and quick procedure
- Does not require microsurgery
- Useful for small anterior tongue defects
- Donor site scar is well-hidden in the cheek fold
- Can be used in medically unfit patients who can’t tolerate long surgeries
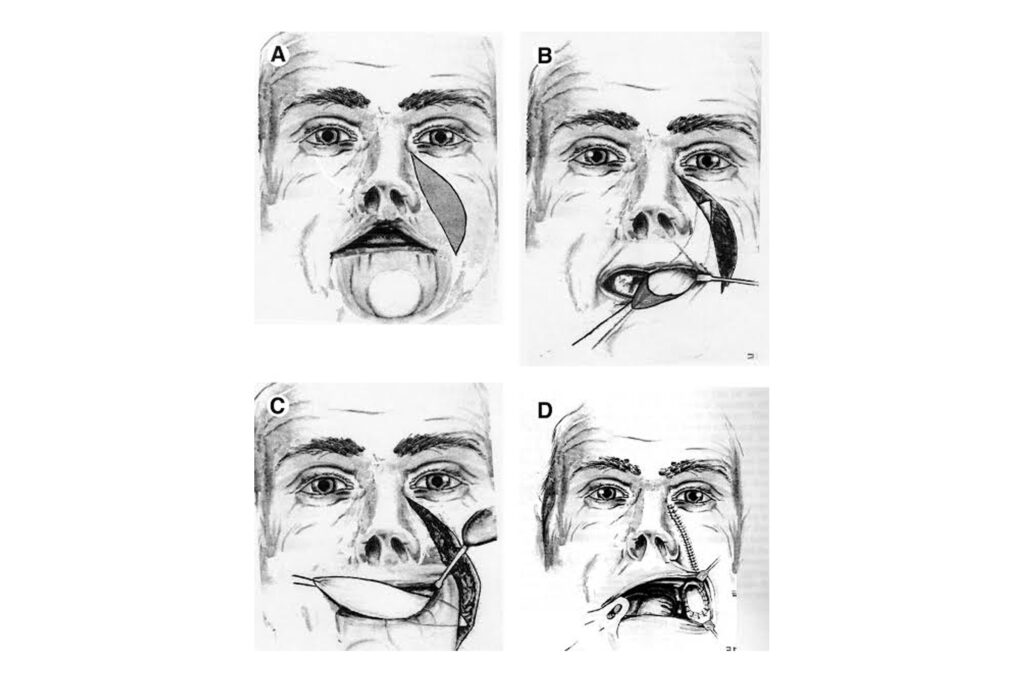
Procedure Steps :
1. Tumor removal from part of the tongue
2. A flap is raised from the cheek fold
3. Flap is rotated or tunneled into the oral cavity
4. Sutured to the tongue defect
5. Donor site closed primarily
Limitations:
- Not suitable for large or posterior tongue defects
- May cause restricted tongue mobility
- Less ideal for functional recovery compared to free flaps
- Can cause oral tightness or cosmetic asymmetry
Best Suited For:
- Elderly or high-risk patients
- Small anterior tongue or floor-of-mouth defects
- When microsurgery is not feasible
Tongue Reconstruction Using PMMC Flap
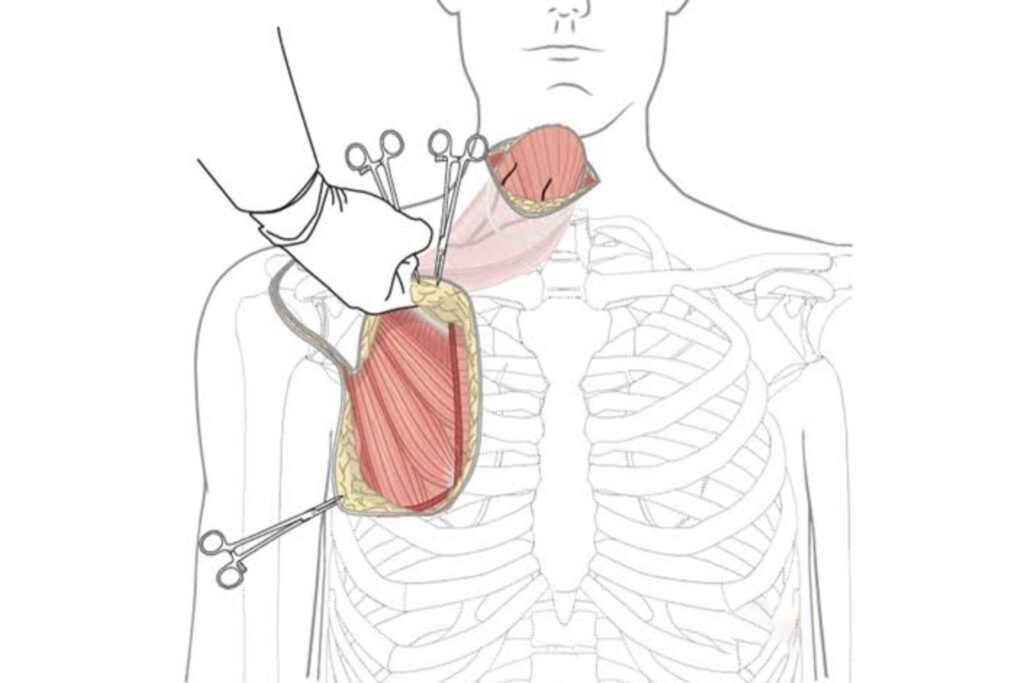
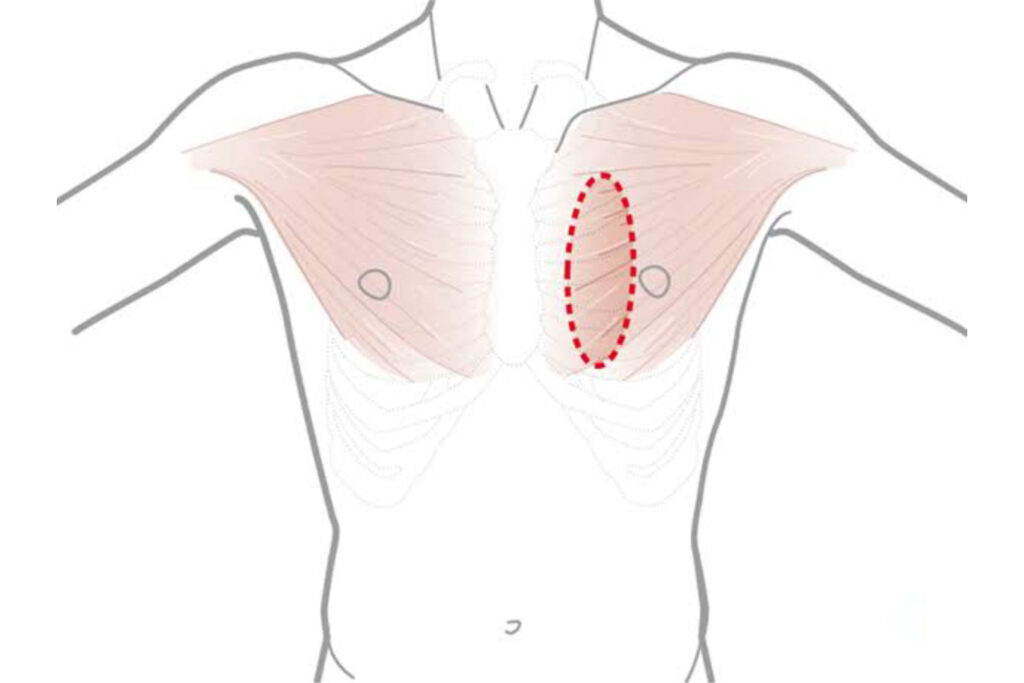
What is a PMMC Flap?
The Pectoralis Major Myocutaneous (PMMC) flap is a pedicled flap taken from the chest
region, including part of the pectoralis major muscle along with overlying skin and fat. It is
rotated into the mouth without microsurgery, making it a robust option when free flap
reconstruction is not feasible.
When is it used?
- In medically unfit patients where microsurgery is risky
- In resource-limited settings
- As a backup flap when free flaps fail
- For large soft tissue defects involving tongue/floor of mouth
Advantages:
- Reliable vascularity
- No need for microsurgery
- Good bulk for filling large defects
- Relatively quick and easy to perform
Limitations:
- Bulky, limits tongue mobility and speech
- Poor cosmetic and functional outcomes
- May impair swallowing and oral hygiene
- Donor site may cause chest wall deformity
Surgical Steps:
1. Tumor is removed from tongue
2. A flap from the chest muscle is raised
3. Flap is tunneled under the skin to the mouth
4. Flap is shaped and sutured to defect
5. Donor site is closed primarily or with graft
Best Used As:
- A salvage option
- For high-risk or elderly patients
- When free flap is not possible
Summary:
*The PMMC flap is a safe but bulky option for tongue reconstruction, often used as a backup or when free flaps are contraindicated. While not ideal for function, it remains a lifesaving reconstructive option in difficult situations.
Get In Touch
Schedule a consultation, ask questions, or explore our expert reconstructive surgery services and compassionate care.